An open letter to Australia's Chief Medical Officer and First Assistant Secretary, Health Economics and Research Division at Australian Department of Health and Aged Care.
At the recent Senate Estimates for Australia’s Community Affairs Legislation Committee, Australia’s top health bureaucrats were once again grilled by Senator Rennick and Senator Roberts about what could be causing Australia’s record excess mortality.
Some key features of the “explanations” offered by Australia’s top health bureaucrats about what exactly has been going on were evident:
We’re looking into it, trust us!;
It was maybe undiagnosed COVID;
Yes, there was some harm caused by vaccines, but it wasn’t statistically significant (yes, seriously, he admitted this);
Correlation isn’t causation;
A BRILLIANT study proves the vaccines have not caused the excess mortality;
The study is now published in the Lancet;
An excellent study clearly demonstrates vaccines provided absolute protection against severe outcomes;
Did we mention the study?
I’ll now pass to my colleague who will mention “The Study” once more!
There are several issues with this study addressed in our previous analysis here:
The vaccines are great! Just ignore those who took a vaccine within 7 days... Or those who had more than four of them... Or those under 65.... Or those who had 1... Just straight out ignore natural immunity. Yes, the vaccines are great.
We should be thankful for lockdowns, border closures, isolation orders, quarantine, QR codes, contact-tracing, curve-flattening, school closures, wasteful government spending and now rampant inflation and excess mortality not seen since WWII because the millions saved by vaccination would have been millions more if not for these interventions.
What will come of the real cost of these interventions in the long-term, not least what we have already observed in the short-term?
But I digress.
As we have previously explored, “The Study” is wrought with problems designed to support the “safe and effective” Paradigm.
Commendably, the authors of the study have presented data within their findings that diverge from the unequivocal conclusion of the COVID-19 vaccines being “safe and effective”.
The study authors and the health bureaucrats who cite its conclusions as gospel, however, need to correct and/or clarify their reliance on this study as the definitive truth that COVID-19 vaccines have not contributed to Australia’s excess mortality in 2022; COVID-19 related mortality; or all-cause mortality.
In sum, the study itself provides evidence of the following:
A higher risk of all-cause mortality among certain cohorts of COVID-19 vaccinated individuals, particularly those who have received two doses, compared to the unvaccinated.
A statistically significant indication of harm from the COVID-19 vaccine in specific cohorts, demonstrated by “negative vaccine effectiveness” where the confidence interval lies entirely below zero.
Therefore, the statements made by Professor Paul Kelly, Australia’s Chief Medical Officer, and Doctor Philip Gould, First Assistant Secretary, Health Economics and Research Division require correction in the public record, or clarification as set out in our open letter, which we have copied below.
Dear Professor Kelly and Doctor Gould,
I write to seek clarification on statements made during the Community Affairs and Senate Estimates on 26 October 2023, concerning the impact of COVID-19 vaccination on mortality rates.
Professor Kelly, in your exchanges with Senator Rennick and Senator Roberts, you made several statements about COVID-19 vaccine safety, referencing the study “Effectiveness of COVID-19 vaccination against COVID-19 specific and all-cause mortality in older Australians: a population based study”. These statements were:
“The study you talked about earlier that's now been published does that. It very specifically looks at who has been vaccinated, using the exact numbers from the Australian Immunisation Register and matching that with ABS related deaths numbers. That is not just PCRs. ABS relies on a doctor writing a death certificate, which will take into account a range of matters. That's the best data we have, and the best data we have shows there is no evidence of an increase in deaths related to vaccination from all causes. If you look at vaccination in relation to over 65s from COVID, they are 88 per cent protected. That's from the same study in early '22.” [emphasis added]
“What we did talk about earlier today is a peer reviewed paper that has now been published that I mentioned at the last estimates. It clearly demonstrates there's no link between the vaccines and all-cause mortality and that there is an extremely strong link between protection from COVID related mortality from vaccination. That is going back to the issue earlier of it being effective. It clearly is effective. It is not associated with this increase in mortality.” [emphasis added]
Dr. Gould, in your exchanges you also stated:
“The study you are referring to found no evidence of increased all-cause mortality associated with COVID vaccines. As you said, it did find a statistically insignificant negative relationship between vaccines and all-cause mortality. It was not statistically significant.” [emphasis added]
“It is important to point out that the study showed that the people who had vaccines were relatively less likely to die of COVID than people who did not have vaccines. That was the key finding of the paper. That was a relative comparison between cohorts of people who had and had not been vaccinated. That in itself doesn't relate to overall mortality rates.” [emphasis added]
However, the study presents data that appear to conflict with these assertions, showing increased mortality risks in specific cohorts and timeframes. This discrepancy calls for a detailed examination and a clearer presentation to the public. As such, I request a comprehensive correction or clarification of the public record in light of the study’s detailed findings.
Professor Kelly, your claims outlined in points 1 and 2 above are contradicted by the evidence presented in the study:
First, there is clear evidence of an increase in deaths from all causesfrom the vaccine compared with those who did not receive the vaccine for the following cohorts:
January-May 2022 study period:
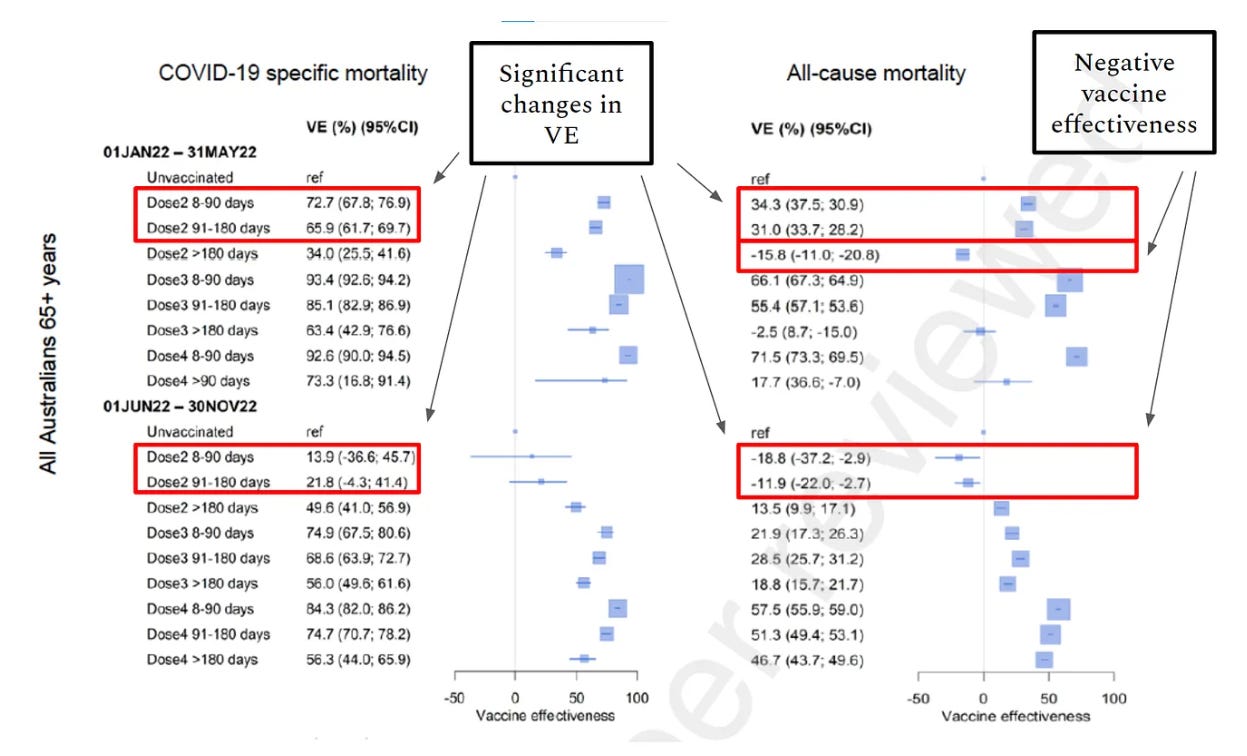
Dose 2 > 180 days: VE estimate of -15.8 (-11.0; -20.8): Showing a moderately increased mortality risk compared with those who did not receive the vaccine.
June-November 2022 study period:
Dose 2 8-90 days: VE estimate of -18.8 (-37.2; -2.9): Showing a moderately increased mortality risk compared with those who did not receive the vaccine.
Dose 2 91-180 days: VE estimate of -11.9 (-22.0; -2.7): Showing an increased mortality risk compared with those who did not receive the vaccine.
Second, there is concerning evidence of negative vaccine effectiveness for the “recent” (8-90 days and 91-180 days) 2 dose cohorts in the study period June-November 2022.
Third, similar negative vaccine effectiveness is evident for the “recent” 2 dose cohorts relating to all-cause mortality in both study periods, and dramatic changes in VE are observed.
Therefore, evidence exists in this study showing evidence of an increase in deaths related to vaccination from all causes.
Evidence in this study clearly demonstrates there is a link between the vaccines and all-cause mortality for some cohorts.
Evidence in this study shows an association with increased mortality for some cohorts.
The study ignores similar and significantly higher mortality rates in these cohorts:
January-May study period:
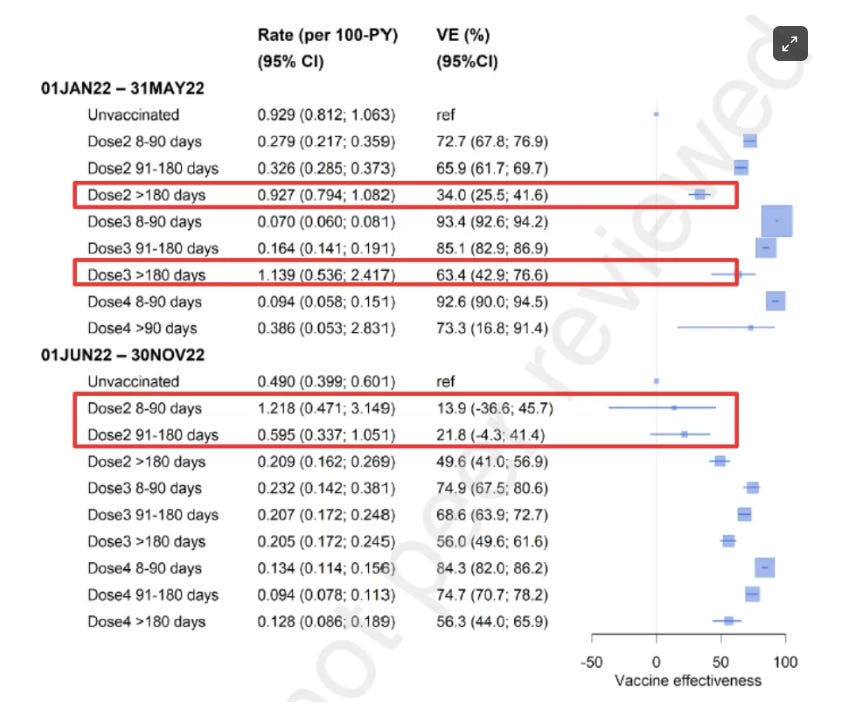
Dose 2 > 180 days: approximately equivalent mortality rate compared with the unvaccinated.
Dose 3 > 180 days: 23% higher COVID-19 mortality rate compared with the unvaccinated (or an 18% lower mortality risk for the unvaccinated compared with this 3 dose cohort).
June-November study period:
Dose 2, 8-90 days: 148% higher COVID-19 mortality rate compared with the unvaccinated (or a 59% lower mortality risk for the unvaccinated compared with this 2 dose cohort).
Dose 2, 91-180 days: 21% higher COVID-19 mortality rate compared with the unvaccinated (or a 17% lower mortality risk for the unvaccinated compared with this 2 dose cohort).
Dr. Gould, your claims outlined in points 3 and 4 are contradicted by the evidence presented in the study:
For the January-May 2022 study period:
Dose 2 > 180 days: A VE estimate of -15.8 with a 95% confidence interval of (-11.0; -20.8) demonstrates a statistically significant increased mortality risk for those who had their second dose more than 180 days ago compared to those who didn't get the vaccine. This is because the entire confidence interval is below zero.
For the June-November 2022 period:
Dose 2 8-90 days: A VE of -18.8 with a 95% confidence interval of (-37.2; -2.9) also indicates a statistically significant increase in mortality risk because, again, the entire confidence interval is below zero.
Dose 2 91-180 days: A VE of -11.9 with a 95% confidence interval of (-22.0; -2.7) signifies a statistically significant mortality increased risk as well since the confidence interval does not cross zero.
These findings should prompt further investigation.
Professor Kelly and Dr. Gould, I kindly request that you either correct, clarify or explain your interpretation of the study in light of the points raised in this letter, which are summarised in the table below:
The discrepancies between your statements and the data presented in the study are concerning and the findings in the cited study demand immediate attention.
Additionally, I respectfully request your assistance in securing access to the AIR-MADIP dataset used in this study for independent analysis, expanding its access to independent researchers not affiliated with government, universities, research institutes or think-tanks. Access to this data is essential for verification and analysis of the results presented and also, to investigate the nature of Australia’s failing health and wellbeing (not just the over 65s, as this study did) as we grapple with the worst excess mortality the nation has encountered since WWII.
I propose that the dataset be made available free of charge, subsidised by the Department of Health and Aged Care. This step would greatly assist in collaborative research efforts to understand and address the underlying factors contributing to Australia's record excess mortality.
Such scrutiny is paramount to maintain public trust and ensure that policy decisions are informed by a complete and accurate understanding of the evidence at hand.