
Consent and the State: Revisiting 2021 (TKQ)
The "vaccination" of TKQ; recommended by a psychiatrist; mandated by the State; against the wishes of his legal guardian: his mother.

On 21 December 2021, the NSW Civil and Administrative Tribunal (NCAT) decided it was appropriate to COVID-19 “vaccinate” “TKQ” to protect him from the grave risks posed by COVID-19 as an “unvaccinated” 62 year-old man living with chronic, untreatable schizophrenia.
The case exposed an inherent contradiction in the relevant legislation.
Consent is personal.
Yet, the legal system must fabricate a substitute version of it when it cannot be given.
Therefore, the “Application for Consent to Medical Treatment” was made by TKQ’s treating psychiatrist, “WBL” and the State “consented” on behalf of TKQ to be “vaccinated” with three Pfizer shots.
The case against the “vaccine”
At the hearing, TKQ’s mother “DZQ” (TKQ’s legal Guardian) and sister (TKQ’s alternative Guardian) gave evidence explaining their objections to the “vaccine”, which, in light of the evidence, were entirely well-founded and reasonably precautionary1:
Not enough was known about the “vaccine” and this carried an unacceptable risk;
Many people they knew had experienced adverse reactions from COVID-19 “vaccination”;
TKQ took powerful medication (Clozapine) which the “vaccine” may not interact well with;
TKQ had a history of kidney cancer and the “vaccine” may cause this to recur;
TKQ was immunocompromised;
The “vaccine” clearly didn’t prevent infection and “vaccinated” people were having to get booster shots;
There was a family history of an adverse reaction to an influenza “vaccine”; and most relevantly,
WBL was not properly qualified to recommend vaccination as he was a psychiatrist.
The case for the “vaccine”
The case for the “vaccination” consisted largely of 2021-era tropes delivered by WBL that failed to venture beyond the “safe and effective” mantra:
TKQ was vulnerable to adverse consequences of a COVID infection due to his mental illness, as well as heavy levels of smoking;
TKQ would be protected from serious illness and death from the “vaccination”, even if it would not prevent infection;
The risk from the “vaccine” was simply and only “transient flu like syndrome”; and,
There was only an “association” between “vaccination” and myocarditis, but it was an “extremely small risk”.
In opining about the risks and benefits of COVID-19 “vaccination” and infection with SARS-CoV-2, WBL ventured well beyond his qualification, and so, he sought the opinion of two infectious disease specialists in support of his application.
The expert evidence
The expert evidence was provided by two infectious disease specialists (“Prof. T” and “Dr. R”).
At the hearing, Dr. R was queried about TKQ’s “suitability” for the “vaccine” given his history with schizophrenia, Clozapine treatment and renal malignancy.
The best case Dr. R could come up with was:
“these are not contradindications to TKQ receiving a COVID-19 vaccine”.2
Hardly a ringing endorsement.
Recalling how medical contraindications to COVID-19 “vaccination” were restricted to so few conditions that not even an adverse event from a previous COVID-19 “vaccine” was a condition which permitted an exemption.
It is little wonder, therefore, that Dr. R could come up with nothing more than “these are not contraindications” in a waste of his presumed “expert” time and knowledge on the matter.
A primary school-aged child with basic literacy and comprehension skills could have read a TGA fact sheet about medical contraindications for COVID-19 “vaccination” and contributed as much “expert” knowledge to the case.
Dr. R could not, it is presumed, speak to the necessity of “vaccinating” TKQ, or it surely would have been included in his evidence and the published findings.
Prof. T.’s endorsement was equally lukewarm:
“[T]he risk of serious adverse events relating to Pfizer are difficult to fully establish (ie. the risk of myocarditis) due to the rates approaching background prevalence levels”3
Another ringing endorsement.
The “risk of serious adverse events . . . are difficult to fully establish” was a soft way of saying “yeah, it’s there and we know about it . . . but I don’t want to [or should not] speculate because I could lose my job.”.
Recalling how doctors were threatened with being suspended or deregistered by the Australian Health Practitioner Regulation Agency following their maligned “position statement” in 2021.
Is it any wonder that so few would have come before NCAT willing to present a heteredox view demonstrating, at the very least, uncertainty?
Prof. T also ignored the concept of additional risk from COVID-19 “vaccines”. The negative effectiveness of the COVID-19 “vaccines”, now shown in many published studies, reveals the further risks TKQ faced with “vaccination”.
By taking three “vaccines”, TKQ had an increased chance of becoming infected with COVID-19 compared with remaining “unvaccinated”.
In that scenario, TKQ was exposed to the “vaccine”-related risk immediately and then still faced the background infection-related risk in the normal course of life, leaving him, on that metric alone, in a worse position than if he had not been “vaccinated”.
In summary, there was no ringing endorsement COVID-19 “vaccine” from either of the experts cited in the findings.
Discussion
The widely-reported “pivotal”, Phase III, randomised, double-blind controlled clinical trial reported in the New England Journal of Medicine on 10 December 2020, excluded people like TKQ: immunocompromised and clinically “unhealthy” (smoking and schizophrenia):
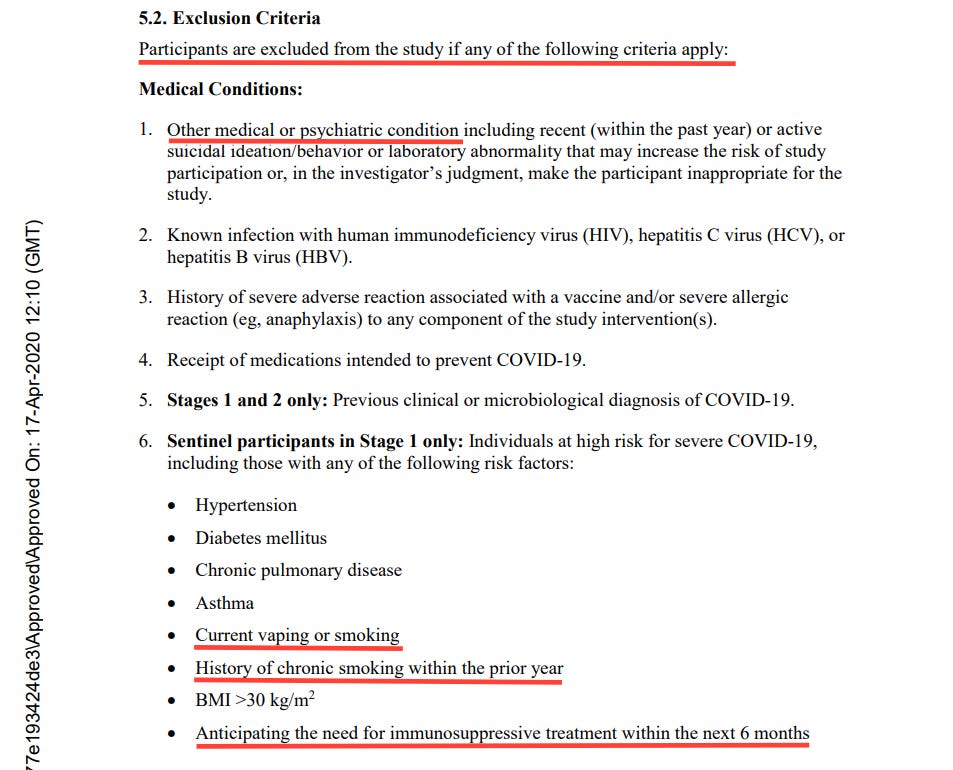
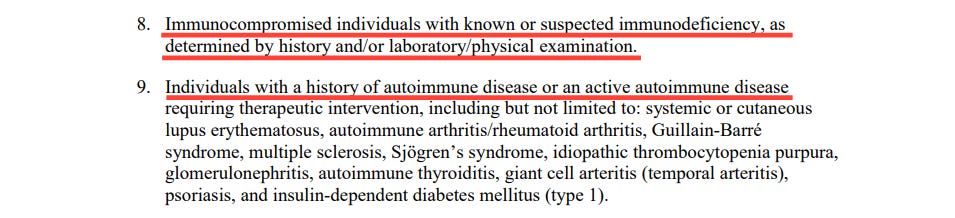
So, even in 2020, it was known that the “vaccine” had not been tested on individuals comparable to TKQ.
It follows that any evidence at the hearing suggesting the “vaccine” was safe for TKQ reflected a serious misunderstanding of the trial data and the limits of the evidence relied upon by those presented as “experts”.
Furthermore, long before the COVID-19 pandemic, a causal association between Clozapine and myocarditis had been established:
It has been estimated that as many as 8% of Clozapine patients in Australia develop myocarditis, though it is more common when commencing treatment. Although TKQ was not commencing Clozapine treatment, this risk of Clozapine-induced myocarditis should have been acknowledged and mentioned by WBL in his evidence to the Tribunal and its omission was, at the very least, careless in the extreme.
The Tribunal member would have surely been swayed by a complete account of the risks of Clozapine coupled with COVID-19 “vaccination”.
Following the conclusion of the case, the risk of Clozapine-induced myocarditis was sufficiently cocerning to prompt NSW Health to issue a “Guideline” called “Monitoring Clozapine-induced Myocarditis”, which explained the clear risks we have elaborated in this article:
As an aside, we infer that this Guideline was likely prompted by “other” unnamed and unacknowledged causes of myocarditis that for some reason may have remained elevated at the time of publication of this Guideline (17 October 2022).
Care to guess what it could have been?
NSW Health were probably loving it that another cause for myocarditis was found.
Nothing to do with another medical intervention.
Funny, isn’t it, how quickly adverse events from a particular medicine can be addressed, even when there is simply the association with the therapeutic.
Such simpler times.
Conclusion
To any casual observer, this should have been an open-and-shut case.
The State affirmed legal guardian — the mother to her child — had decided what was best for her ward/charge — her son.
Her family had all agreed with the decision to decline the proposed treatment, as was their legal right and obligation.
The fact that the Tribunal gave any consideration or weight to WBL’s evidence is deeply concerning. Although the Tribunal member noted deficiencies in the legal or medical arguments put forward by TKQ’s family (mother, sister and brothers), WBL was largely given a free-pass with very little interrogation of his ambit claims about COVID-19 risks and “vaccine” benefits (let alone necessity).
On the evidence presented in her findings, the Tribunal member’s decision was swayed by the “expert” evidence resulting in her granting of “consent” for the “vaccination” of TKQ.
Had WBL provided a complete account of the risks and benefits of what he was qualified (we hope?) to speak about — Clozapine — “consent” may never have been granted.
In her findings, the Tribunal member could have written the following explaining why the State should not have “consented” to the “vaccination” of TKQ:
“Medical procedures are rarely risk free, and decisions about medical treatment inevitably involve balancing the risk of the treatment, the risk of not having the treatment, and the benefit of having the treatment. For example, a low risk procedure which provides significant benefit and alleviates a risk of deteriorating health would usually be a situation where the balance is in favour of the procedure going ahead. Alternatively, a high risk procedure, which provides questionable benefit, addressing a condition which causes little impairment, is likely to be a situation where the balance is in favour of not proceeding with the treatment.”4 [emphasis added]
This was precisely what she wrote explaining her decision to “consent” for TKQ to be “vaccinated”.
Her reasoning was sound; she just inverted the conclusion.
Even if the Tribunal member disagreed with the evidence that COVID-19 “vaccination” was a high risk procedure, it was established at the time of the case that it provided questionable benefit(s).
It was known that the “vaccine” did not prevent infection and, likely worse, made you more susceptible to infection (and the possibility of the clinical progression of COVID-19 illness).
Even if the Tribunal member agreed that COVID-19 was a real threat to TKQ, she ignored the extensive evidence of “vaccine” failure that emerged in 2021 which forced those pushing a “safe and effective” narrative to pivot to “it was only ever meant to protect against serious illness and death”: a complete lie which Arkmedic has recently exposed.
As we and many other writers have investigated, the claims about reductions in serious illness and death could have only been made with extraordinarily malevolent data trickery, rendering these assertions also completely meaningless.
Finally, COVID-19 was indeed a disease that caused “little impairment” in the majority. Even with grossly exaggerated counts of “COVID-19 deaths”, the case-fatality rate showed COVID-19 was non-lethal for the absolute majority.
On the evidence at NCAT, however, it seemed that the Tribunal member was unable to disentangle her assumptions about COVID-19’s risks from the benefits of the “vaccine”. If she believed the evidence put to her that COVID-19 was a risk for the majority, then she had already decided that it did not cause “little impairment” and, therefore, justified her decision to “consent” for the “vaccination” of TKQ.
It is a pity that her findings were based, in part at least, on cartoonish talking points about COVID-19 from a psychiatrist masquerading as an “expert” on vaccines and epidemiology who was either unable (or unwilling) to provide information that was crucially relevant to the case from his own field of presumed expertise.
Final thoughts
If the State must intervene to “consent” on behalf of a person that cannot, then there must be extraordinary grounds for doing so and, on the facts presented in the case, the threshold was not even close to being met.
And therein lies the real problem.
A man who could not “consent” to a necessary medical treatment was literally mandated to be “vaccinated” against the wishes of his mother, sister and brothers.
He could not consent.
He did not consent.
Children, too, cannot meaningfully “consent” to “vaccination” in the way described in the case of TKQ, it could be argued.
Is it too far-fetched to think, that at some point in the future, the State argues that your decision to choose not to “vaccinate” your child was tantamount to “neglect” or “abuse” and that the risks of a certain pathogen (real or imagined) outweighed your rights to make informed health choices for your own child?
What could be scraped from your metadata to discredit you in any relevant way to show you were a consumer or purveyor of “misinformation” or “disinformation” to really make the case that the State should decide what is right for your child?
What is right for you?
What is right for us?
The case of TKQ should be illustrative as to what the future holds and the necessity of being prepared against the threat of government overreach into the lives of our most precious loved ones.
Under the Guardianship Act 1987, a “Guardian” means a person who is a guardian of the person of some other person (other than a child who is under the age of 16 years), and includes an enduring guardian. “Guardianship orders” are applied for and made in hearings at NCAT and DZQ had been his legal Guardian for many years as described at [4] in her findings: “been subject to guardianship orders made by this Tribunal for many years and his mother, DZQ has consistently been appointed guardian. The guardianship order was reviewed and renewed on 12 February 2020 and DZQ was reappointed for two years with authority to make decisions for TKQ regarding his accommodation, services, health care, medical and dental consent. His sister, “Ms. Z”, was reappointed as the alternative guardian. TKQ has another sister, “Ms. Y”, and a brother, “Mr. X”, TKQ [2021] NSWCATGD 23
I have 2 adult kids with Down syndrome and have been writing about eugenics since they were born 20+ years ago now. 2020 was a deja-vu moment for me and I immediately pulled them out of school (they were still in school back then).
As we've seen before, the vulnerable are at the frontlines of the depopulation because a. the perps can easily get away with it by blaming it on their 'condition' or 'vulnerability', b. people with disabilities/chronic illness etc. are portrayed as a (financial) burden and c. while the perps hate all of us, they hate the vulnerable (who bring out our soft and caring side) the most.
While society at large is told to take these shots to protect the vulnerable, the vulnerable are given extra shots because of their so-called vulnerability.
Thanks for your article.
The entire medical profession, and the wider general Public (including the Judiciary) projected what they *wanted to believe* onto this thing. They did ZERO due diligence.
Couple extreme ignorance with the hubris and arrogance of these characters, across several sectors, and it ensured they got it completely wrong - grossly mismanaging what would've been over in 3-4 months, and instead turning it into a years-long medical, social, and economic disaster.