
Herding Consent: The School Vaccination Program (Part 1)
The quiet failure to obtain valid, informed consent in NSW Health's School Vaccination Program.

Prior to the COVID-19 pandemic, we never would have critically reflected on the importance of routine childhood vaccinations and the importance of staying “up-to-date” with safe, effective and necessary vaccinations.
After all, you didn’t want to be an “anti-vaxxer”. Those people were outcasts.
Could you really question the most important breakthrough in modern medical history? The one solely responsible for the remarkable advances in life expectancy and living standards?
In the pre-COVID era, you didn’t have to think about these things.
Vaccines didn’t cause autism.
Propaganda made it easy not to think about these things too deeply:
After all, didn’t you know…
Yes.
They sure do.
Just in the same way that…

In the post-COVID era, however, with our eyes well and truly now opened, it has become apparent that propaganda, disinformation and censorship were not just methods deployed by the State and its legacy media about COVID “vaccines”; rather, this had been ongoing for years with Australia’s National Immunisation Program (NIP) and we just weren’t aware.
Propaganda about the benefits of vaccines.
Censorship of the harms of vaccines.
Disinformation with the two put together.
Nowhere is this more apparent than with Australia’s School Vaccination Program. The Program’s propaganda fails to provide the parents of school-aged children — let alone the children themselves — with sufficient, accurate and comprehensible information to provide valid, informed consent to receive the vaccines on offer.
Informed consent requires a clear understanding of both the potential risks and benefits of a given vaccine, as well as the relative risk posed by the disease it is designed to protect against or prevent.
As our investigation will show, this standard is not being met in NSW Health’s School Vaccination Program.
Remarkably, the Parent Information Sheet distributed to parents as part of the Program fails even to mention the specific vaccine used.
The omission of this key detail raises serious questions about the legality of the consent obtained by NSW Health as part of the process.
What is informed consent?
The Nuremberg Code was a set of ethical research principles established in 1947 after the Nuremberg Trials, specifically the Doctors’ Trial, to prevent the recurrence of inhumane medical experiments like those conducted by Nazi doctors during World War II.
Though it didn’t create the notion of “informed consent”, it was the first major international document to formalise and mandate it as an absolute ethical requirement in human experimentation:
“The voluntary consent of the human subject is absolutely essential. This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment. The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.”1 [emphases added]
The COVID-19 “vaccine” experiment — the world’s largest clinical trial — was an unmistakable breach of this principle; particularly once coercive “vaccine” mandates were imposed.
Yet, what about routine, no longer “experimental” or approved childhood vaccines?
So-called “routine” childhood vaccinations are somewhat different from the COVID-19 “vaccines” as they are licensed and “fully approved” by our courageous regulator (who approves a mere 90% of their sponsors’ applications for new medicines; receiving a paltry 96% of their budget from sponsors’ fees) and are, therefore, classified as standard medical care: not experimentation.
Despite their differences to the COVID-19 experimental “vaccines”, however, these routine childhood vaccines of course also require valid, informed consent before they can be administered.
Informed consent and routine childhood vaccination
The legal foundation for informed consent in Australia is grounded in common law, compelling a medical practitioner to disclose all material risks, those a reasonable person in the patient’s position would consider significant, alongside the nature, purpose, and alternatives to the proposed treatment.2
Consent must also be voluntary and based on an adequate understanding of these risks and benefits. While written consent is recommended for invasive procedures, vaccination typically involves verbal or implied consent, provided it meets the “informed” standard as described in the Australian Health Practitioner Regulation Agency’s “Good Medical Practice: A Code of Conduct for Doctors in Australia”:
Similarly, the Australian Medical Association also reinforces that informed consent must be freely given, specific, and based on sufficient information for all medical care, including vaccination, adopting guidelines recommended by the Australian Commission on Safety and Quality in Health Care:
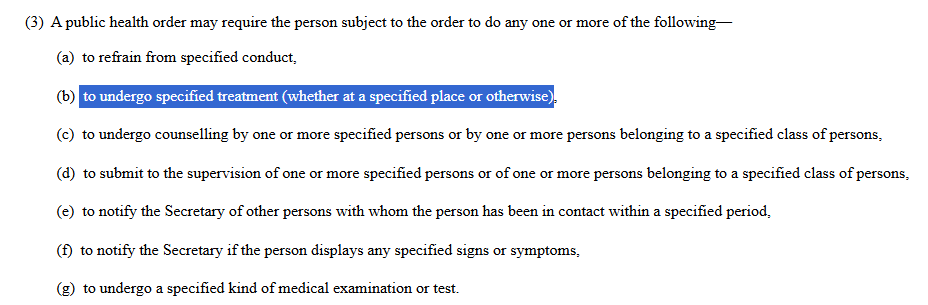
Even in an alleged “emergency”, in New South Wales for example, informed consent could only be overridden in very limited circumstances under the Public Health Act 2010 (NSW). Section 118 permits the Chief Health Officer to issue a public health order requiring a person to undergo medical examination, treatment, test or isolation if they are suspected of having a serious infectious disease classified as a Category 4 or 5 condition — which could have hypothetically included COVID-19:3
There are, therefore, very limited conditions under which “informed consent” can be overridden, even during public health emergencies.
Informed consent in the School Vaccination Program
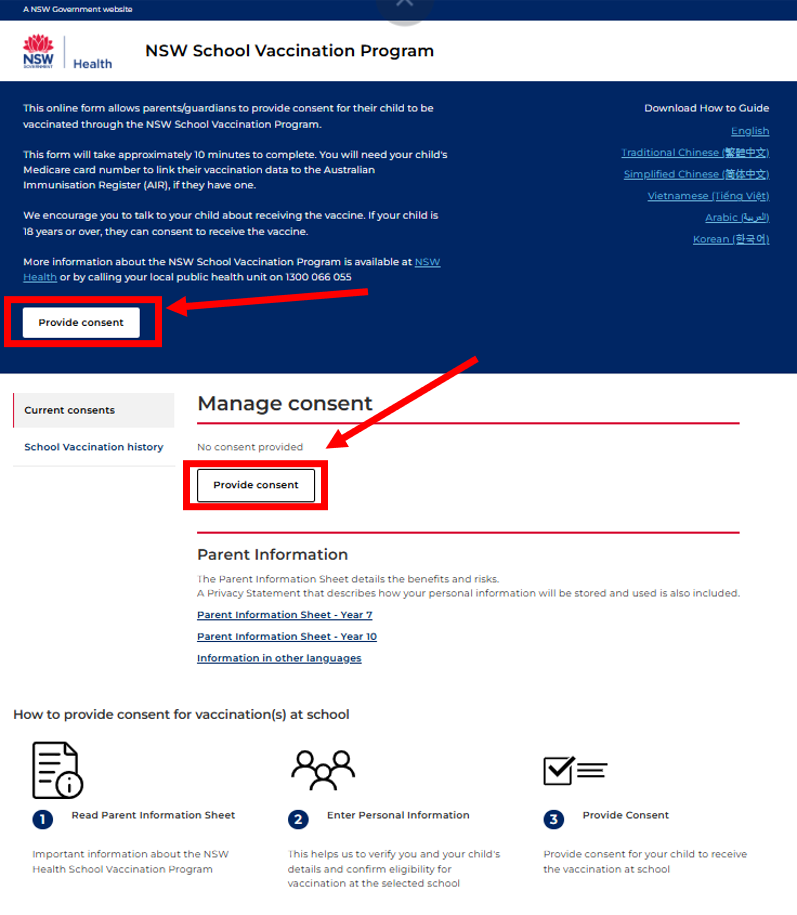
We now illustrate the typical process-flow for providing consent for your child to be vaccinated in NSW Health’s School Vaccination Program.
You can follow this process too by going to Service NSW School Vaccination Program and logging in with your Service NSW credentials.
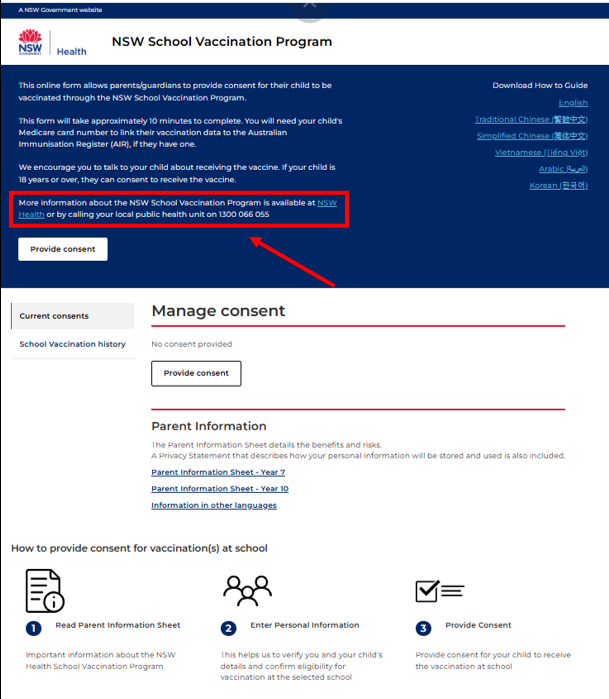
Step # 1 - Click the above link and login to your Service NSW account and click either of these buttons to take you to the consent page
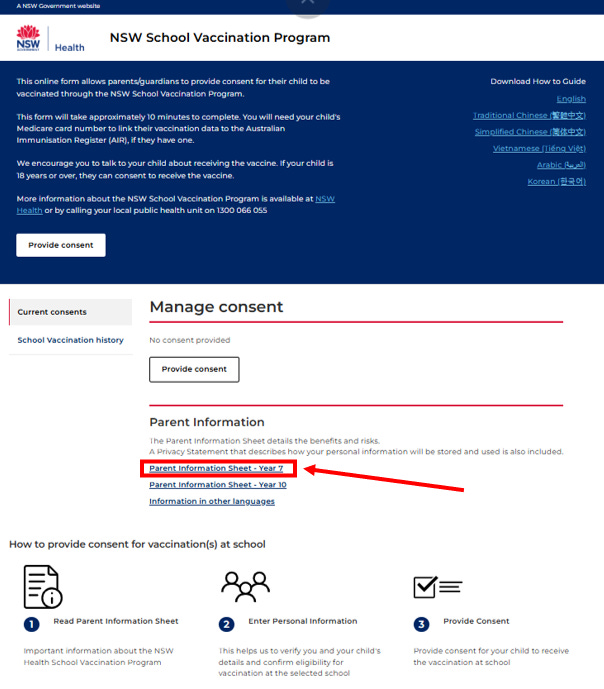
Step # 2 - If you’re not comfortable providing consent, you can click the “Parent Information Sheet” link to hopefully learn more about these vaccines on offer:
Which opens up to this document showing a group of elated unvaccinated students (inferred from their ability to raise what must be unjabbed arms):

Step # 3 - Review the Parent Information Sheet:
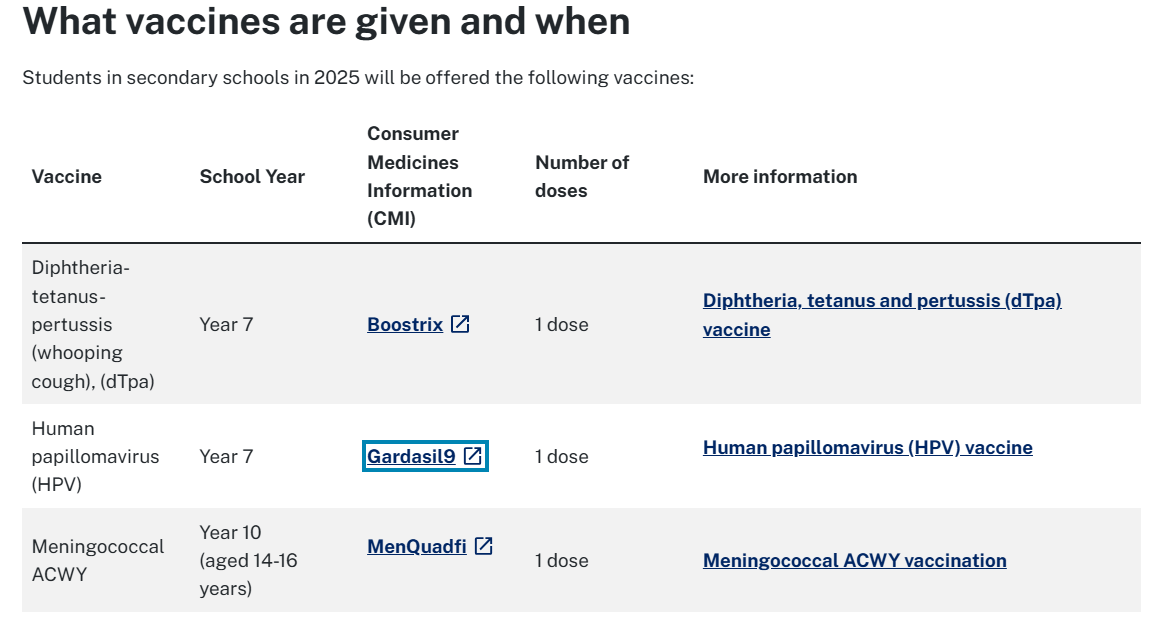
The first page reminds us that Experts have recommended the vaccines (two are given to Year 7 students in NSW as part of the School Vaccination Program):

The second page is a list of very basic questions about vaccines in general, or the simple process to providing consent to have your child receive them:
“How do vaccines work?…
How safe are vaccines?…
What are the side effects of vaccination?…
What is anaphylaxis?…
What if my child has asthma and takes cortisone or prednisone by a “puffer”?
The vaccines can be safely administered to someone who has asthma regardless of which medications they are taking.
Should the vaccine be given to a female student who is or thinks she may be pregnant?
No. Any female student who is, or thinks she may be, pregnant should not be vaccinated. On the day of the clinic the vaccination nurse will ask female students if they are or could be pregnant. If a student answers yes to this question, she will not be vaccinated. The student will be urged to immediately discuss the issue with her parent/ guardian and to seek medical help. She will also be provided with contact details for a health referral service that will provide advice, support and guidance.
Can I withdraw consent?…
What if I prefer to wait until my child is older?…
What if my child missed out on the vaccine at school?…
Can students with physical and/or intellectual disabilities be vaccinated at school?…
How can I access a record of the vaccinations?…
Where can I find more information about school vaccination?…” [emphases added]
Notice how few of these have anything to do with the specific vaccines (“Gardasil 9” or “Boostrix”) offered?
Only two of the questions pertain to the vaccines offered to Year 7 students as part of the program, and only one contraindication is noted — pregnancy.
The following pages — “information about each of the vaccines” — details the risks of Human Papillomavirus (HPV) and its role in causing approximately 5% of all cancers worldwide (we will address the vaccine for Diphtheria-Tetanus-Pertussis in a separate article):
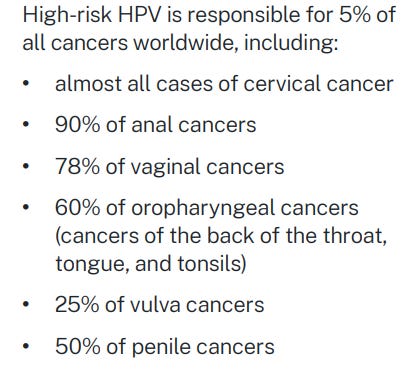
Yet the information sheet fails to clearly explain the difference between these long-term cancer risks in adults and the much lower short-term risk to 12–13 year olds of these cancers. It also does not mention how rare these cancers are in young people or that 90% of HPV infections clear on their own. Overall, it gives the impression that serious illness is an immediate risk to children which warrants — it is assumed — vaccination protection from infections caused by HPV.
But it is important to note that Gardasil 9 does not even cover all HPV types. There are over 200 types of HPV and 14 of those are considered “high-risk” because they are oncogenic. Nine types of HPV are targeted by Gardasil 9 (hence the name), but only seven targeted by the vaccine are considered “high-risk” (the other two are “low-risk”, targeting genital warts). Seven of these other “high-risk” types, though less-common, are not targeted by the Gardasil 9 vaccine. This is acknowledged in the section “Who should be vaccinated?”, but the brochure exaggerates both the risks of HPV and the benefits of the Gardasil 9 vaccine, therefore not providing appropriate information for parents and children to make an informed choice.
The information sheet also lacks any citations or references, making it hard for parents to verify the information — particularly when alarming claims of 100% protection are made:
Perhaps the most egregious error is that the name of the vaccine is not given anywhere in the Parent Information Sheet.
It is simply referred to as “[a]n HPV vaccine…”:
The vaccine in question is, of course, “Gardasil 9”.
Merck, the manufacturer of Gardasil 9, has an alarming track-record when it comes to meeting its legal obligations regarding the safety of its products, which also extends to Gardasil 9.
As reported by investigative journalist Maryanne Demasi, Merck misled the participants in one of the clinical trials for Gardasil 9, compromising the rights of those in the placebo group to informed consent by injecting them with an active and non-safety tested adjuvant to make placebo outcomes appear worse than in the vaccinated group.
Merck is also the same company which distorted its clinical trial data for Gardasil 9 so thoroughly that the results were rendered scientifically meaningless, concealing an adverse event rate of 3.3% of its 14,000 participants in one clinical trial; in a follow-up window that was limited to only 14 days.
Gardasil 9 has also been found to contain residual DNA fragments which could cause cancer and has ingredients that can act as transfection agents which Merck was aware of and lobbied regulators to help them bypass testing requirements.
The omission of the vaccine name “Gardasil 9” from the Parent Information Sheet, is therefore, an omission which seriously calls into question whether “informed consent” could have possibly been obtained for the administration of the Gardasil 9 vaccine in the School Vaccination Program.
Step # 4 - Try and find some more information
If unsatisfied with the information, you can visit the NSW Health page by clicking the link shown:
Which takes you to this page where you can click on the tab “For parents and carers”
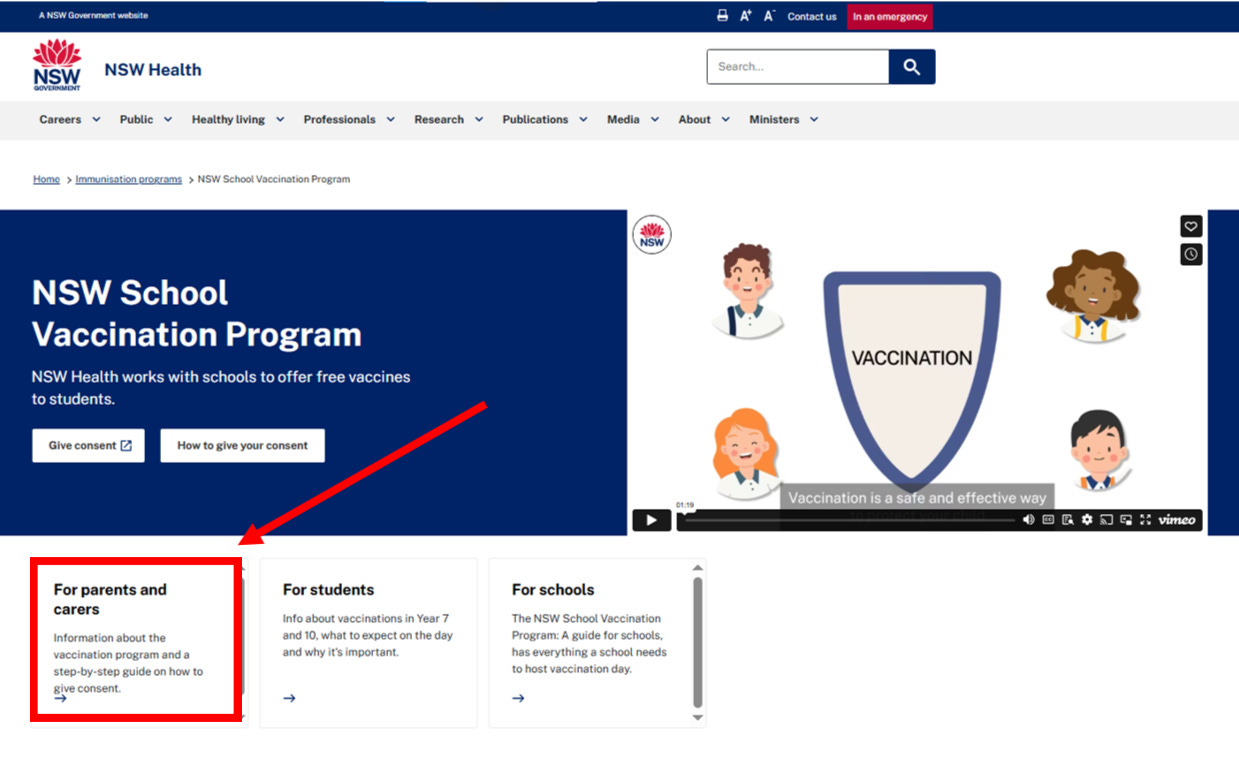
Which takes you to a page providing more information about the expected reactions and risks following vaccination with Gardasil 9.
Finally, this is the first instance where the actual names of the vaccine(s) is (are) provided:
Clicking the “Gardasil 9” link takes you to its Product and Consumer Medicine Information License where more information about the actual vaccine is provided, however, it is limited to barely more than five pages of information in a brochure-styled presentation:

And once again, no citations are provided to support the claims made in this brochure, in what is essentially a condensed version of the TGA’s Australian Public Assessment Report for Gardasil 9, which does not address the serious risks of Gardasil 9, including death.
Step # 5 - Provide consent?
At this point, you are directed to declare you have availed yourself of the information in the Parent Information Sheet to the extent required to “understand the benefits and risks of vaccination” — generally it would seem — and to confirm that you consent to the vaccine(s) offered:
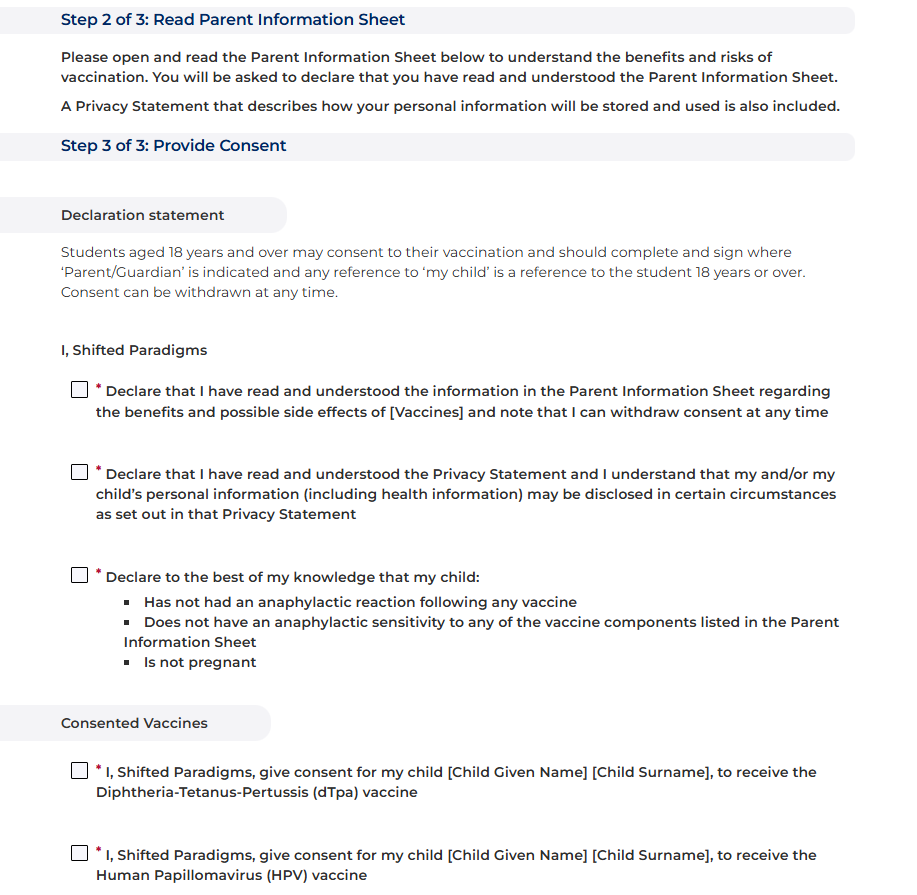
Once these boxes are ticked and the online form is submitted, then “informed consent” is considered to have been obtained.
Discussion
The opaque process of NSW Health’s School Vaccination Program challenges whether valid and informed consent could have possibly been obtained for these medical procedures.
The School Vaccination Program’s website obscures critical details, requiring navigation through multiple pages to simply even identify the vaccine(s) in question. The website information provides only vague assurances about safety and benefits without age-specific risk data for 12–13-year-olds.
Given cervical cancer’s low mortality rate (approximately 250 deaths annually in Australia) and effective screening, the necessity of vaccinating pre-adolescents against HPV is questionable, particularly in light of concerns about residual DNA plasmids and Merck’s clinical trial practices, which used non-saline controls to make exaggerated claims about safety, efficacy and risk.
The necessity of the vaccine and its role in reduced cervical cancer incidence is also subject to debate. It is suggested that the National Cervical Screening Program is responsible for the reduction in cervical cancer incidence than the Gardasil quadrivalent and Gardasil 9 vaccines:
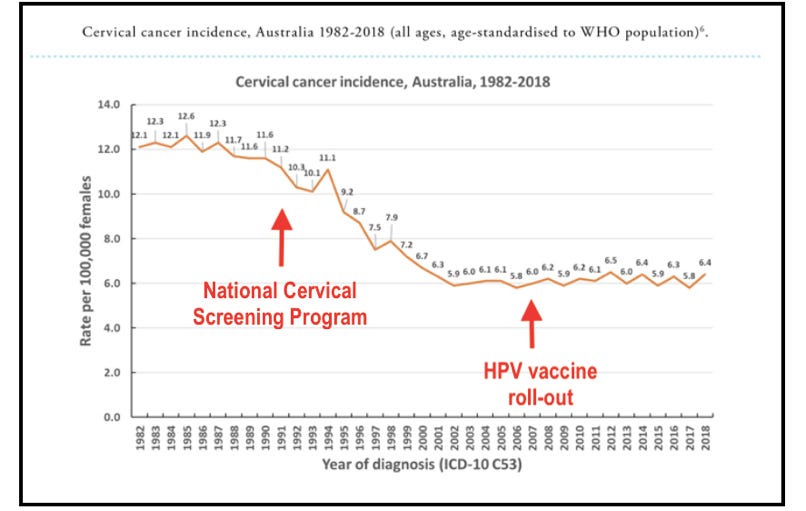
As these cancers would take decades to develop in older cohorts, it remains to be seen if these rates of cervical cancer (among others) will reduce even further in the coming decades.
It is, however, important to remind our readers that Gardasil 9 neither protects against all HPV-induced cancers, nor is HPV the only cause for these cancers. As the above chart reveals, the National Cervical Screening Program is the most likely cause of the reduction in the most commonly associated HPV infection-induced cancer: cervical cancer.4
So why do we vaccinate at schools?
The School Vaccination Program ensures that vaccines like Gardasil 9 are efficiently delivered, obtaining high coverage across the 12-13 year old population, reducing the administrative burden that it would place on general practitioners (GP) to do so for these tens of thousands of students and their parents.
But it also is a deliberate ploy to normalise the process, making it seem like an administrative process akin to handing in a permission slip; thereby dulling the sense of medical risk that each vaccination entails.
When everyone is doing it, resistance feels abnormal. Students don't want to be the odd one out, and parents are less likely to refuse if they believe refusal is rare.
GPs are trained to obtain informed consent, answer questions, and assess patient suitability. Bypassing them reduces the chance of hesitancy being triggered by actual dialogue about risks and benefits.
Despite sliding rates of vaccination coinciding with the pandemic (approximately 83% to 70% from 2019-2023 in NSW):
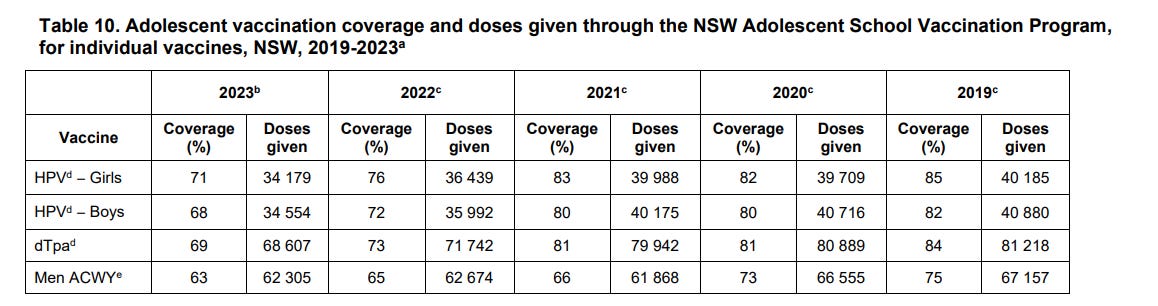
tens of thousands of mostly Year 7 students in NSW alone have been vaccinated each year with Gardasil 9 each year in this period. The parents of these “vaccinees” would have undergone the same consent process outlined in this article.
Based on what we have shown, how many of the parents providing consent could we estimate were properly informed of the risks of HPV infection, the rates of cancers resulting from HPV infection, survival rates of cancers caused by HPV infection, the benefits of Gardasil 9, the risks of Gardasil 9 and the necessity of Gardasil 9 for their child?
How much more likely would it be that the majority of these parents simply checked the boxes to provide consent as directed?
We must remember that all medicines produce effects.
The ones we aim for are called benefits and the ones we don’t want are called side effects.
But they are all part of the same trade-off and Gardasil 9 is no different.
Remember when five girls fainted after being immunised at school (when the original Gardasil was first rolled out)?

It was just a coincidence of course:
“But authorities said their reactions were likely to be related to having an injection, not the vaccine itself. . . . Sacred Heart Girls' College headmaster Christopher Dalton said hospital staff told teachers at the school at the time that the girls' reactions were not related to the vaccination itself.”5 [emphasis added]
The vaccine was safe and effective:
“Mr Abbott agreed, saying manufacturer CSL had tested the vaccine batch in question and found it ‘perfectly fit and proper’ . . . Mr Abbott said Gardasil was vigorously evaluated before being registered for use in Australia and it had passed with flying colours.”6
Millions of doses had been given and Experts would have noticed something because they’d have done something about it if there was a risk, because they were the Experts:
“No other Australian adverse reaction cases had been brought to his attention.
In the United States, where the vaccine had undergone a similarly rigorous evaluation and been in use longer, two million people had been vaccinated and only 500 reactions reported, he said.”7
Do you remember when three women developed pancreatitis after being injected with the original Gardasil?
It was probably just another coincidence too.
In fairness, with so many doses of Gardasil and Gardasil 9 given, we should expect elevated rates of adverse events, but how just how many?
What’s the risk profile we accept for incomplete protection against an infection which only may cause cancer, for which even if it does occur, the survival rates are very positive?
Gardasil and now Gardasil 9 have been associated with 3 deaths and over 4,400 reports of harm in 12-17 year olds in Australia as reported in the TGA’s Database of Adverse Event Notifications (DAEN):
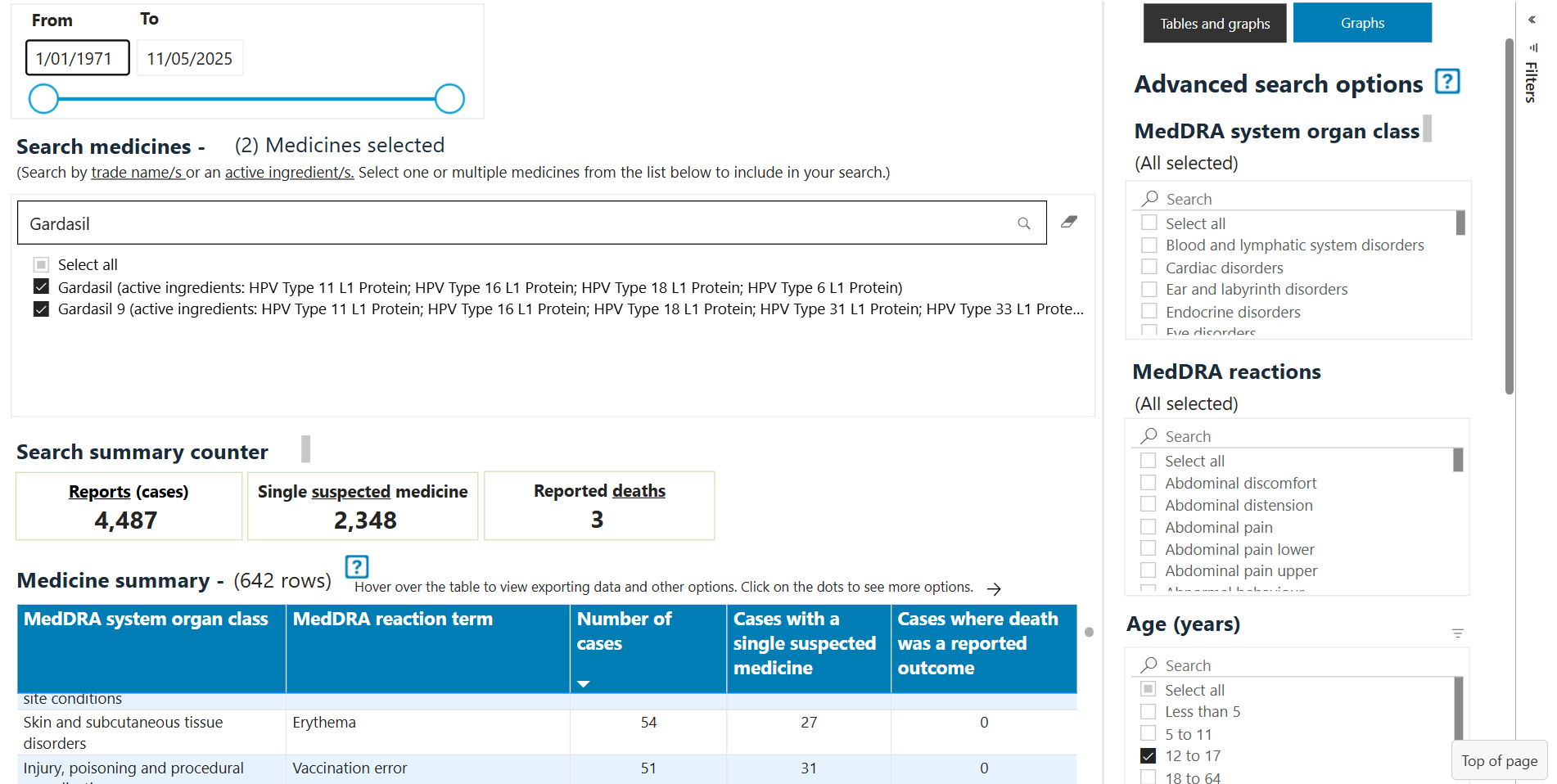
Clearly, this vaccine is not completely safe.
The signal in the data shown above is even more relevant because 12-17 year olds tend to be in the prime of their lives health-wise and would not otherwise expect to be reporting ill-health unless it was for the vaccine they had received.
In sum, it is highly likely that these adverse event reports to DAEN were likely more than mere coincidences associated with vaccination.
Sadly, the three reported deaths associated with Gardasil 9 (following its rollout in 2018) all occurred in children only 12 years old.
Two of these deaths include “Boostrix” in the “Medicines reported as being taken” report, suggesting that these children would have received their vaccines as part of the School Vaccination Program:
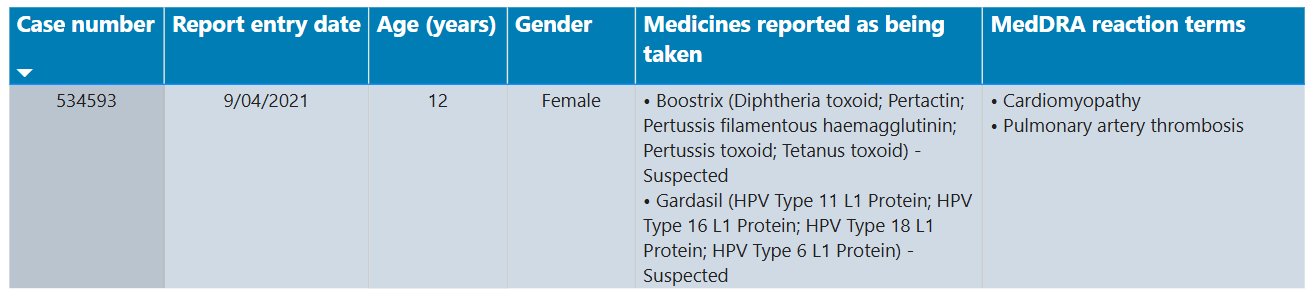
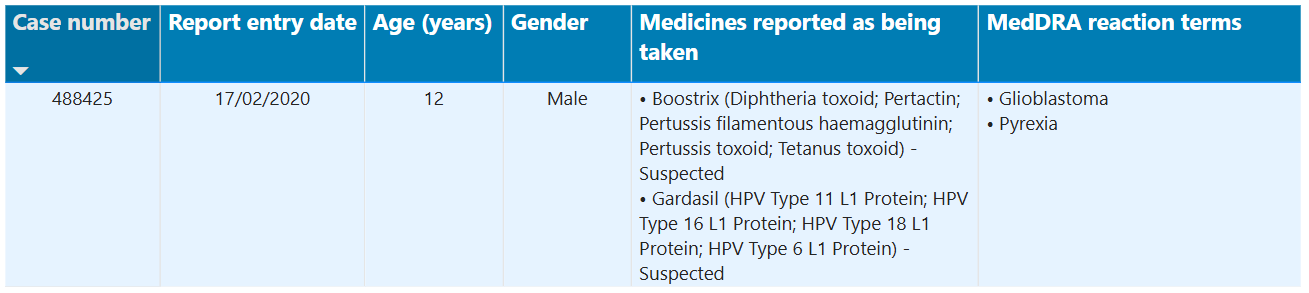

How sad if these three children died because their parents provided “consent” through a tick-box portal without being fully informed of the risks of this vaccine.
Though the number of adverse events and deaths might appear relatively small considering the number of doses given, due to the under-reporting ratio, these numbers could possibly be 99% higher than recorded in DAEN.
Conclusion
Informed consent requires a clear understanding of both the potential risks and benefits of a given vaccine, as well as the relative risk posed by the disease it is designed to protect against or prevent.
Australia’s School Vaccination Program has failed parents and children by providing them with insufficient information about the risks of HPV, the benefits of vaccination with Gardasil 9 and the risks of vaccination with Gardasil 9.
The consent obtained by Australia’s health authorities may, therefore, be considered unlawful and it could amount to assault, battery, or negligence.
If you are the parent of a child due for vaccination with Gardasil 9, then pause and withhold consent until adequate, relevant and comprehensible information is provided.
Request full disclosure, including the name of the product, known risks, alternatives and expected benefits of Gardasil 9 from your GP or school vaccinator.
Ask critical questions such as “what are the short-term and long-term effects of Gardasil 9 and is this vaccine necessary for my child?”
Keep written records of what information was provided, what was asked, and what was withheld.
If key information is missing, then submit formal complaints to educational authorities, health departments and the Ombudsman.
Thank you for reading.
Trials of War Criminals before the Nuremberg Military Tribunals under Control Council Law No. 10. Nuremberg, October 1946–April 1949. Washington, D.C.: U.S. G.P.O, 1949–1953, https://en.wikisource.org/wiki/Nuremberg_Code, accessed 21 May 2025.
Rogers v Whitaker (1992) 175 CLR 479, 489 (Mason CJ, Brennan, Dawson, Toohey and McHugh JJ).
Public Health Act 2010 (NSW) s 62
See:
Vieira-Baptista, P., "Risk of Development of Vulvar Cancer in Women With Lichen Sclerosus or Lichen Planus: A Systematic Review", Journal of Lower Genital Tract Disease, Vol. 26, No. 3, https://screeningforlife.ca/wp-content/uploads/Vieira-Baptista-P.-et-al-2022-Risk-of-Development-of-Vulvar-Cancer-in-Women-with-Lichen-Sclerosus-or-Lichen-Planus.pdf
Department of Health and Aged Care, “Smoking and Cervical Cancer”, https://www.health.gov.au/our-work/tobaccofacts/smoking-and-cervical-cancer, accessed 24 May 2025.
The Sydney Morning Herald, “Parents Urged Not to Panic over Gardasil”, https://www.smh.com.au/national/parents-urged-not-to-panic-over-gardasil-20070522-e5m.html, accessed 25 May 2025.
Ibid.
Ibid.
Thank you for your work SP.
As an aside, I had to 'log in' to Substack twice to interact with your article - once to 'like' the post and once more to comment.
Shifted Paradigms, you say: “GPs are trained to obtain informed consent…”
Are GPs trained to obtain informed consent?
Exactly what training do they receive in this area?
Given that GPs vaccinate under coercion and mandates, eg under No Jab, No Pay/No Play and COVID-19 vaccine mandates, it seems to me they are clueless about valid voluntary informed consent for vaccination.
Also see: Just ‘following orders’? https://elizabethhart.substack.com/p/just-following-orders