
Sedation, Not Salvation (Part 3)
Substantial increases in palliative care prescribing coincides with record excess mortality in residential aged-care facilities.

Introduction
Given the widespread failures, neglect, and systemic issues exposed during the Royal Commission into Aged Care Quality and Safety, it was expected the severe mismanagement and understaffing would cause devastating COVID-19 outbreaks in residential aged-care facilities (RACFs) in 2020.
To some extent, these fears materialised but not to the level predicted by many. Though Australia’s “COVID-19 deaths” mostly occurred in RACFs in 2020, as we demonstrated in Parts 1 and 2 of this series of articles, these “COVID-19 deaths” were likely the result of prematurely prescribing and administering sedatives which hastened residents’ deaths “from COVID-19” among other leading causes such as dementia.


In 2021, however, the story quite unexpectedly changed.
While the rest of the nation (primarily in NSW and Victoria) dealt with an explosion in “COVID-19 cases” with the Delta wave, somehow Australia’s RACFs managed to not only restrict “COVID-19 deaths” but “COVID-19 cases” too.
In 2021, there were just 282 “COVID-19 deaths” and 1,737 “COVID-19 cases” in Australia’s RACFs from approximately 242,000 individuals living in permanent RACFs in Australia.1
Why did the older and more comorbid aged-care residents have better COVID-19 infection and mortality outcomes than the rest of the Australian population in 2021?
Was it natural immunity from prior infections?
Did the RACFs get their act together and learn how to respond to and manage COVID-19 in 2021?
Was it the “vaccines”?
In this article, we interrogate the reasons for these unexpected outcomes in Australia’s RACFs and show how the low number of “COVID-19 deaths” in 2021 was a calm before the storm of the Omicron wave.
We will show how soaring rates of prescribing for sedatives and opioids on the PBS’s (Pharmaceutical Benefits Scheme) Palliative Care Schedule, which paled in comparison to our analysis of 2020’s data, caused record excess deaths in Australia’s RACFs from late 2021 onwards.
Why were residents in aged-care facilities better off in 2021?
Was it natural immunity?
With a relatively low number of “COVID-19 cases” in RACFs 2020-21, natural immunity would not have been sufficiently widespread to explain the reduction in “COVID-19 cases” and “COVID-19 deaths” in 2021.
In non-outbreak scenarios in 2020, COVID-19 testing was reduced, raising the possibility that non-severe “COVID-19 cases” were missed, leading to underestimations of the true number of “COVID-19 cases” and therefore, the extent of natural immunity in the RACF population. Conversely, hyper-sensitive PCR-testing methods could have caught more “COVID-19 cases” than had meaningfully existed possibly leading to overestimates of natural immunity as well.
In 2021, however, it is likely that more “COVID-19 cases” were captured through a massive expansion in testing in RACFs. By 10 August 2021, 475,170 COVID-19 tests had been completed at 2,544 unique residential aged care facilities RACFs nationally.2
Yet, as protective as natural immunity could have been, it could have only minimally accounted for these improved infection and mortality outcomes, as case numbers were so low in 2020 and 2021.
The comparably worse outcomes for RACF staff from 2020 to 2021 (addressed in the next section) further disproves the natural immunity explanation for lower “COVID-19 cases” and “COVID-19 deaths” in RACFs in 2021.
Did Australia’s RACFs get their act together?
In 2021, RACF resident “COVID-19 cases” and “COVID-19 deaths” sharply declined. There were 14% fewer resident “COVID-19 cases” and 68% fewer resident “COVID-19 deaths” compared with 2020.3 Similarly, there were 58% fewer RACF staff “COVID-19 cases” than in 2020, yet unexpectedly, 13 staff succumbed to “COVID-19 deaths” (up from zero) in 2020.4
The striking reductions for COVID-19 infections and mortality in RACFs bucked the trends for the wider Australian population, where both “COVID-19 cases” and “COVID-19 deaths” started to significantly trend upwards from June 2021 onwards.
There is evidence, therefore, that Australia’s RACFs learned from the mistakes of 2020, and applied stricter and more consistent infection control measures to explain lower “COVID-19 cases” and “COVID-19” deaths in 2021. These RACF protocols included restricting visitor access, mandatory testing for staff, better infection control monitoring and reporting, and more timely information sharing with health authorities.5
Yet, the extent to which these measures were responsible for better COVID-19 outcomes in 2021 must have been limited considering how these same processes failed from 2022 onwards, when both “COVID-19 cases” and “COVID-19 deaths” once again soared in Australian RACFs, resulting in more than 3,200 “COVID-19 deaths”.6
Was it the “vaccines”?
The extent to which it was “vaccination” that explained, or at least partly explained the unexpected reduction in the number of aged-care “COVID-19 cases” and “COVID-19 deaths” depends on vaccine coverage and timing of the receipt of “vaccines”, and the prevalence of COVID-19 in Australia at the time.
“Vaccination” coverage and timing in RACFs
Although aged-care residents were eligible to be “vaccinated” much earlier than the rest of the Australian population, the data show that “vaccination” coverage was lower in the RACF cohorts compared with the Australian population overall. By the end of 2021, only 87.2% of residents in aged-care facilities had been “double vaccinated” compared with 90.2% of the Australian population aged 12 and over;7 a modest increase from the 85.3% reported to have been “double vaccinated” by early July 2021.8
There was also limited “vaccination” coverage for RACF staff, even until after the “vaccine” mandate took effect on 17 September 2021 for all RACF staff. In June 2021, it was reported that only 16.3% of RACF staff were “fully vaccinated”, with only 30% having received one dose. By 16 September 2021, vaccination rollout data revealed that only 78.1% were “fully vaccinated” and a month later this had risen to 91.8%.9 In sum, COVID-19 “vaccination” coverage was not sufficiently widespread and was also slow to achieve for RACF staff.
With so many unwashed, “unvaccinated” RACF staff potentially superspreading COVID-19, the “vaccination” coverage was insufficient and could not explain the improved infection and mortality outcomes in Australia’s RACFs in 2021.
Three fanciful assumptions of the idea that “vaccines” could have played any role in the reduced infection and mortality in RACFs in 2021 are:
The “vaccines” could prevent infection;
The “vaccines” reduced your risk of repeated COVID-19 infections; and,
The “vaccines” were safe and did not cause elevated mortality from other (non-COVID-19) causes.
All of these assumptions are false.
Timing of “vaccination”
As shown in the previous section, residents in aged-care facilities reached a high-level of “vaccination” coverage (85.3%) earlier in 2021 than the rest of the Australian population and, therefore, the presumed protective effects of the “vaccine” could not explain the improved infection or mortality outcomes in Australia’s RACFs in 2021.
The study “Effectiveness of mRNA Vaccines and Waning of Protection Against Sars-CoV-2 Infection and Severe COVID-19 During Predominant Circulation of the Delta Variant in Italy: Retrospective Cohort Study” showed “vaccine”-effectiveness waned substantially to the point where six months after “vaccination” high-risk (aged over 60 years) were no better off than the “unvaccinated”:
“At 27-30 weeks after the second dose, vaccine effectiveness was estimated to be similar to no protection in high risk people.”10
Negative vaccine effectiveness has been demonstrated in multiple other studies, most notably in this Australian study which we wrote about in 2023, showing how some cohorts were more likely to die “from COVID-19” or from other leading causes than the “unvaccinated”.
Therefore, any presumed benefits from “vaccination” would have waned considerably if the primary course was completed at the time of the rollout in February 2021.
“Vaccination” does not, therefore, explain the improved COVID-19 infection and mortality outcomes in RACFs in 2021.
The prevalence of COVID-19 in Australia in 2021
In the first half of 2021, Australia experienced very low numbers of “COVID-19 cases”, with most infections linked to international arrivals in hotel quarantine. Community transmission was rare and typically contained. It wasn’t until mid-June 2021 that the Delta variant triggered a major outbreak, beginning in Sydney and marking the start of prolonged lockdowns and a significant national case surge (see below: note the graph uses a logarithmic scale to show “new ‘COVID-19 cases’” as they were barely visible on a linear scale prior to August 2021):
The story was very similar in RACFs. The first “COVID-19 Outbreaks in Australian Residential Aged Care Facilities” report for 2021 showed that a cumulative total of only 2,027 “COVID-19 cases” (all from 2020) had been recorded in RACFs increasing to just 2,032 on 26 June 2021; still with zero “COVID-19 deaths” by this time. By 30 July 2021, cases had increased to 2,060; still with zero deaths. It was not until the report from 13 August 2021, that the first “COVID-19 deaths” were reported and the number of “COVID-19 cases” escalated to 2,113, (86 added in 2021 to the 2,027 from 2020).
The lack of “COVID-19 deaths” or “COVID-19 cases” when there was no community transmission disproves the claim that “vaccines” caused this outcome. It simply shows there was no exposure to COVID-19 in RACFs in the first half of 2021, with “healthy vaccinee bias” leading to the misconception that it was the protective benefits of “vaccination” which was responsible.
Whilst “COVID-19 deaths” might have been low during this period, it would be wrong to assume that all “vaccine” recipients were healthy in this period (January to 13 August 2021; when the first “COVID-19 deaths” were recorded). The staggering numbers of adverse events reported in the TGA’s Database of Adverse Event Notifications — underreported by as much as 99% — shows the true impacts of the “vaccines” for the aged 65+ cohort:
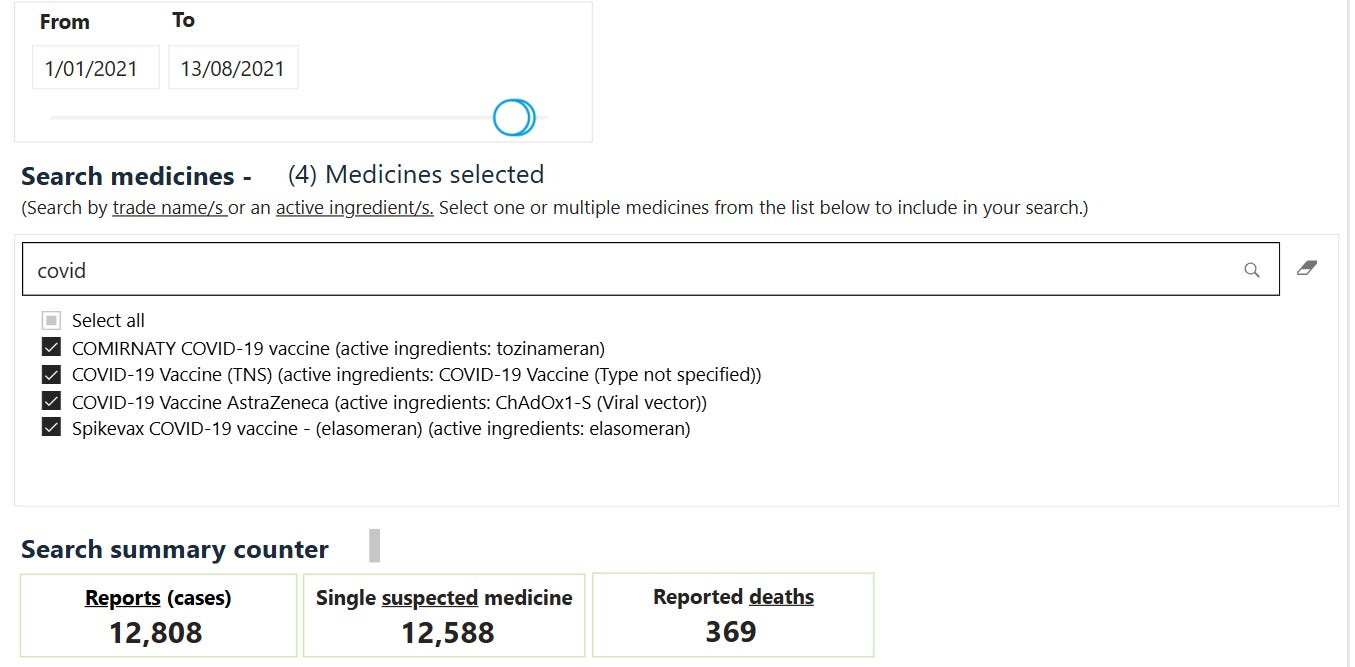
In sum, “vaccination” did not cause the relatively positive COVID-19 infection and mortality outcomes in RACFs in 2021. “Vaccine” coverage was relatively limited for residents, slow to achieve for RACF staff and any presumed “vaccine” effectiveness would have waned considerably by the time of the Delta wave for RACF residents. With low COVID-19 prevalence in the community, any positive outcomes were the result of the “healthy vaccinee bias” which glosses over the serious reported harms, including deaths from all COVID-19 “vaccines” in the period from January to 13 August 2021; when the first “COVID-19 deaths” in RACFs for 2021 were reported.
Soaring palliative care prescribing in June 2021 onwards
Here the story turns.
Starting in June 2021, there was a sharp increase in the prescribing of sedatives and opioids on the PBS’s Palliative Care Schedule. These substantial increases resulted from a Department of Health review in February 2020, which brought about changes to the PBS Palliative Care Schedule, expanding access to medicines used in palliative and “end-of-life” care which were formerly restricted to cancer patients only.
Aside from expanding access to these medicines, other restrictions were also eased following the review. Special authority requirements were simplified and the number of repeats, quantities and dosages were also increased for these medicines.11 The increased volumes of medicine dispensed, due to larger quantities and repeats per prescription, meant that the explosion in the number of sedatives and opioids was a much larger increase, by medicine volume or quantity, in comparison with the pre-June 2021 prescribing data.
The graphs below show alarming increases in sedative and opioid use, which, given the data is publicly viewable on the PBS Date of Supply data, must have occurred in outpatient or RACFs (not in hospitals):12
Expanded and simplified access to palliative or “end-of-life” care sedatives and opioids can explain how prescribing could have occurred, but does not address why it should have.
The perfect storm
With expanded access to sedatives and opioids as part of palliative care and “end-of-life” prescribing, coupled with an explosion in “COVID-19 cases” in the Omicron wave, RACFs experienced soaring excess mortality.
Not all of these excess deaths were “from COVID-19”, but a large proportion were.
As we demonstrated in Parts 1 and 2 of this series of articles, palliative and “end-of-life” medicine prescribing spiked in the period immediately preceding or matching rises in “COVID-19 deaths”.
Below we present similar data for 2020-23, showing increased prescribing together with “COVID-19 deaths”, which is particularly evident during the peak of the Omicron wave. The red shaded area highlights the spike in prescribing in December 2021 followed by the rise in “COVID-19 deaths” in January 2022 (this will not be visible in your email, please click the graph to open it in a new window):
The sharp increase in prescriptions in December 2021 does not reflect stockpiling behaviour because it continued the upward trend that began in June 2021, maintaining consistency with the heightened demand already evident in months prior, rather than showing a sudden, isolated spike typical of stockpiling.
Note the corresponding drop in palliative care prescribing which occurs in January 2022, suggesting that the approximate 380 “COVID-19 deaths” in RACFs in January 2022 significantly curbed the demand for “end-of-life” care medicines because these residents had succumbed to sedation, or “COVID-19 deaths”.
Though “COVID-19 cases” in RACFs were relatively low in 2021, they were mostly recorded later in the year. Approximately 1,340 were reported in the period between 24 September to 24 December 2021 and this influx of “COVID-19 cases” in RACFs — just as it did in 2020 — was likely to have led to many being placed on the “end-of-life” protocol involving these sedatives and opioids.13
There are other evident spikes in prescribing either preceding or matching spikes in “COVID-19 deaths” after December 2021-January 2022; however, with only monthly data available for prescribing it is not presently possible to calculate by how much, if at all, these prescribing spikes preceded the “COVID-19 deaths”.
Record excess mortality in residential aged-care facilities
There is more to our analysis than elevated “COVID-19 deaths” in RACFs.
A 2023 study which compared mortality rates in RACFs across a number of years, found that there were 4,896 excess deaths in the period July 2021-June 2022 which accounted to 21% of the national excess deaths, even though those in RACFs represented less than 1% of the Australian population.14
The study used publicly available data from financial years, tracking the number of permanent residents and “exits” (deaths) in RACFs, and so its study period included both the peaks of the Delta and Omicron COVID-19 waves, somewhat complicating our calendar year analysis so far.
Though our analysis here focuses on data from calendar years, we were able to piece together data from the Department of Health “COVID-19 Outbreaks in Residential Aged-Care Facilities” reports. We know that the majority of these “COVID-19 deaths” in RACFs did not occur in the Delta wave having established the very low numbers of “COVID-19 deaths” in RACFs in 2021 (282 or approximately 22% of the national “COVID-19 deaths” for that year).
As addressed previously, the first “COVID-19 deaths” occurring in RACFs were the three reported in the 13 August 2021 report, meaning all 282 “COVID-19 deaths” in 2021 must have occurred in the period from August-December 2021 — within the study period (July 2021-June 2022). The report from 1 July 2022 shows 2,881 “total COVID-19 deaths” had occurred “since the beginning of the pandemic”, meaning that 1,921 “COVID-19 deaths” must have occurred in the period from January to July 2022 in Australia’s RACFs.15
In sum, from July 2021 to June 2022, there were 2,203 (1,921 + 282) “COVID-19 deaths” and 2,693 non-COVID-19 excess deaths in RACFs.
Interpreting residential aged-care excess mortality
Excess dementia mortality is the likely reason for the elevated non-COVID-19 excess deaths in the study period. Compared to the 2015-19 average, there were 2,294 excess dementia deaths in 2021 and 3,468 excess dementia deaths in 2022.16 Though this is a crude estimate not accounting for changes in the age-structure of the population in that time, these are strikingly large excesses which would only minimally be reduced by any changes in demographics in this short period of time. These are likely even underestimates because the mortality displacement caused by elevated deaths in 2021 should have reduced the deaths in 2022, but the reverse was observed.
As Australia’s population ages, dementia has become an increasingly common comorbidity in Australia’s RACFs. Data from the Australian Institute of Health and Welfare (AIHW) shows that in the study period (July 2021 to June 2022), there were approximately 131,000 people living with dementia (54% of all residents) in RACFs. In an outbreak scenario, with so many suffering with the disease in RACFs, those residents at an advanced stage of the disease could have been prescribed and administered these palliative and “end-of-life” care medicines as infection control measures, possibly causing these excess dementia deaths. While the approach would have reduced “COVID-19 deaths” in RACFs, these same sedatives and opioids, at the individual level, could have deepened confusion, slowed breathing and raised fall risks, accelerating decline in people with dementia and leading to elevated “dementia deaths”.
In a likely genuine coincidence, another AIHW report calculated that approximately 4,800 residents in RACFs (roughly 2% of all residents) were appraised as needing palliative care in this same study period (July 2021 to June 2022); a remarkably close alignment with the reported 4,896 excess deaths.17 Though, in reality, the numbers accessing palliative and “end-of-life” care would be much larger as virtually all residents close to death would access these medicines at some point before their eventual deaths.
Conclusions
In 2021, there was an expansion in access to palliative and “end-of-life” care medicines — sedatives and opioids — which coincided with record excess deaths in Australia’s RACFs.
The evidence presented in this article shows a continued need for these medicines that outlasted COVID-19 waves.
As we wrote earlier in the article, this is not simply about expanded and simplified access to these medicines, it is about why they should have been needed.
Something has made Australians sicker and it has not only persisted, but worsened since 2021, requiring more and more sedatives and opioids.
What could have caused the significant jump in the numbers of people requiring access to palliative care and “end-of-life” care medicines in 2021?
Was it simply a coincidence that the Department of Health commissioned a review in February 2020, just as the pandemic kicked-off, seeking ways to get more sedatives and opioids into Australians?
Was it yet another coincidence that Australia’s excess mortality crisis commenced at just the same time that these sedatives and opioids became available to many more Australians?
Had our pain-relief needs really been unmet for so long until these important changes?
Or did these changes reflect something more sinister?
Was it just another coincidence — or perhaps strategic convenience — that palliative and “end-of-life” medicines became more readily available, in greater quantities and with weaker oversight, precisely as the Delta wave began?
Was this Australia’s quiet purge of high-cost, low-survival residents under the veneer of “care”; a convenient solution to the “problem” of an ageing population?
So many questions.
We will keep asking.
Thank you for reading.
AIHW, “Dementia in Australia”, https://www.aihw.gov.au/reports/dementia/dementia-in-aus/contents/aged-care-and-support-services-used-by-people-with/residential-aged-care, accessed 13 April 2025.
Department of Health, “COVID-19 Outbreaks in Australian Residential Aged-Care Facilities”, https://www.health.gov.au/sites/default/files/documents/2021/08/covid-19-outbreaks-in-australian-residential-aged-care-facilities-13-august-2021_0.pdf, p. 6, accessed 14 April 2025.
Department of Health statistics reveal that by the end of 2020, there was a total of 2,027 resident “COVID-19 cases”, 1,349 recovered “COVID-19 cases” and 678 “COVID-19 deaths”. By the end of 2021, the total resident cases had risen to 3,764 (an addition of only 1,737 “COVID-19 cases”) and only 282 “COVID-19 deaths” were recorded in Australia’s RACFs. See data for the last reports in December for 2020 compared with 2021 here: https://www.health.gov.au/resources/collections/covid-19-outbreaks-in-australian-residential-aged-care-facilities. The final “COVID-19 deaths” figure for 2021 is reported in this document: https://www.health.gov.au/sites/default/files/documents/2022/02/covid-19-outbreaks-in-australian-residential-aged-care-facilities-25-february-2022.pdf , footnote # 2 on p. 1, accessed 15 April 2025.
Presumably more deaths occurred between the publication of the last report for 2021 and final counts.
By the end of 2020, 2,237 staff “COVID-19 cases” resulted in 2,236 “recoveries” at the time of reporting (December 2020), with one active case remaining (suggesting a possible 100% recovery rate). Yet, 2021 added only 946 more staff “COVID-19 cases” resulting in 745 “recoveries”, with 189 active cases at the time of reporting (December 2021). The difference in total cases (which includes “active cases”) and recoveries for the staff in RACFs suggests that perhaps as many as 13 staff “COVID-19 deaths” had occurred in 2021.
The significant reduction in “COVID-19 deaths” in 2021 is most likely even an underestimate. Two footnotes in the 2021 Department of Health report “COVID-19 outbreaks in Australian residential aged care facilities” show that the data likely even overestimated the low COVID-19 mortality in RACFs in 2021. These footnotes define a “COVID-19 death in NSW and in Victoria (the two states where the majority of Australia’s “COVID-19 deaths” occurred) as either a death from a clinically compatible illness (NSW) or a death that occurred within 28 days of a positive COVID-19 test result was categorised as a “COVID-19 death” (Victoria). These two footnotes do not appear in the 2020 report suggesting that in 2021 especially, “COVID-19 deaths” in RACFs were overestimated given this flimsy methodology. See here: Department of Health and Aged Care, “COVID-19 Outbreaks in Australian Residential Aged Care Facilities”, https://www.health.gov.au/sites/default/files/documents/2021/12/covid-19-outbreaks-in-australian-residential-aged-care-facilities-23-december-2021.pdf, page 1, footnotes 2 and 3, accessed 9 April 2025.
Department of Health, “Protecting Older Australians: COVID-19 Update 8 January 2021”, https://web.archive.org/web/20221118064419/https://www.health.gov.au/news/newsletters/protecting-older-australians-covid-19-update-8-january-2021, accessed 13 April 2025.
Welsh, J., Joshy, G., Freeman-Robinson, R., Biddle, N., Banks, E., Schlegel, C., Jordan, K., Gould, P., Kelly, P. and Korda, R., “Understanding the Fatal Burden of COVID-19 in Residential Aged Care Homes in Australia: Using Linked Data to Generate Evidence”, International Journal of Population Data Science, 9(5), 2024. doi: 10.23889/ijpds.v9i5.2691.
Department of Health and Aged Care, “Australia’s COVID-19 Vaccine Rollout”, https://www.anao.gov.au/sites/default/files/2022-10/Auditor-General_Report_2022-23_3_0.pdf, p. 6, accessed 9 April 2025.
Department of Health, “Press Conference in Melbourne on 5 July 2021 about a Mandated Vaccination for Aged Care Workers, the Vaccine Rollout and a COVID-19 Update”, https://www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/press-conference-in-melbourne-on-5-july-2021-about-a-mandated-vaccination-for-aged-care-workers-the-vaccine-rollout-and-a-covid-19-update, accessed 13 April 2025.
The Medical Journal of Australia, “Implementing Mandatory COVID-19 Vaccination in Aged-Care Workers”, https://www.mja.com.au/system/files/2022-11/FINAL%2021%20NOV%20VAX%20MANDATE%20FINAL.pdf, p. 1.
Fabiani M, Puopolo M, Morciano C, Spuri M, Spila Alegiani S , Filia A et al. “Effectiveness of mRNA Vaccines and Waning of Protection Against Sars-CoV-2 Infection and Severe COVID-19 During Predominant Circulation of the Delta Variant in Italy: Retrospective Cohort Study”, BMJ, 2022; 376 :e069052 doi:10.1136/bmj-2021-069052
Pharmaceutical Benefits Advisory Committee, “Palliative Care Schedule (Pcs) Review and Outcomes of Stakeholder Consultation”, https://www.pbs.gov.au/industry/listing/elements/pbac-meetings/psd/2020-09/files/palliative-care-schedule-review-psd-september-2020.pdf, accessed 14 April 2025.
See also, PBS, “Schedule of Pharmaceutical Benefits Summary of Changes”, June 2021, https://www.pbs.gov.au/publication/schedule/2021/06/2021-06-01-general-soc.pdf, accessed 14 April 2025.
Inpatient prescribing on the PBS is not publicly available or published.
“COVID-19 cases” on 24 December 2021 were 3,764, an increase from 2,424 on 24 September 2021 as reported in the COVID-19 Outbreaks in Residential Aged-Care Facilities reports. See here: https://www.health.gov.au/resources/collections/covid-19-outbreaks-in-australian-residential-aged-care-facilities, accessed 15 April 2025.
Inacio MC, Davies L, Jorissen R, Air T, Eshetie T, Mittinty M, Caughey G, Miller C, Wesselingh S, “Excess Mortality in Residents of Aged Care Facilities During COVID-19 in Australia, 2019–22.” International Journal of Epidemiology, 2024 Feb; 53(1). doi: 10.1093/ije/dyad168.
The report for 1 July 2022 strangely refers to “total deaths” which could include staff “COVID-19 deaths”. In prior reports, staff and resident “COVID-19 deaths” and “COVID-19 cases” were reported separately. It is unlikely they would be bundled together in this report, but these would only minimally impact our analysis if they were.
ABS, “Provisional Mortality Statistics - Deaths by Month of Occurrence 2015-23”, https://www.abs.gov.au/statistics/health/causes-death/provisional-mortality-statistics/jan-dec-2024/Deaths%20by%20month%20of%20occurrence%2C%202015-23.xlsx. The average dementia deaths in the period from 2015-19 was subtracted from total dementia deaths for 2021 and 2022.
AIHW, “Dementia in Australia”, https://www.aihw.gov.au/getmedia/60d5d0da-fd52-4962-ae7d-d1692c3a7433/dementia-in-australia.pdf?v=20241212190340&inline=true, accessed 15 April 2025.
AIHW, “Palliative Care Services in Australia”, https://www.aihw.gov.au/reports/palliative-care-services/palliative-care-services-in-australia/contents/summary, accessed 15 April 2025.
friend, I am so sorry about what Australians have suffered the past several years. I followed with shock and dread the stories I was able to find about your situation. Being in the Midwest of the US information was limited; but I used to have a friend in Oz, so the place occurs to mind more often than others just for that reason. Thank you for you diligent work in compiling and especially analyzing these reports. You raise some crucial questions.
I have some similar personal griefs from 'the Covid time", & some harms are ongoing even now.
out of all my family members, both natural and by marriage, only 4 listened to my concerns about the sh0t. Helplessness I think eventually can produce anger, and that at least can produce the strength one needs to survive. I can't do much now but am dreaming of escaping into the woods someday...
Nice work, had thought it was just the UK with there murder by Midazolam but obviously not.
Personally the consideration of deliberately euthanasing the elderly should be considered. If so there would be policy changes to allow this and the new standard of care would enable the killing because we know know the "care" fields are basically unthinking autonomous scum.
ps
Please consider having graphics that can be downloaded as I'll be sharing your article in all the Facebook groups I'm in and graphics catch the eye.